The phrase "robotic surgery" conjures images of an autonomous machine wielding a scalpel while the surgical team watches from behind glass. That picture is wrong, and it is worth correcting early, because the misunderstanding causes real anxiety for patients who are offered a robot assisted procedure.
A surgeon, always in control
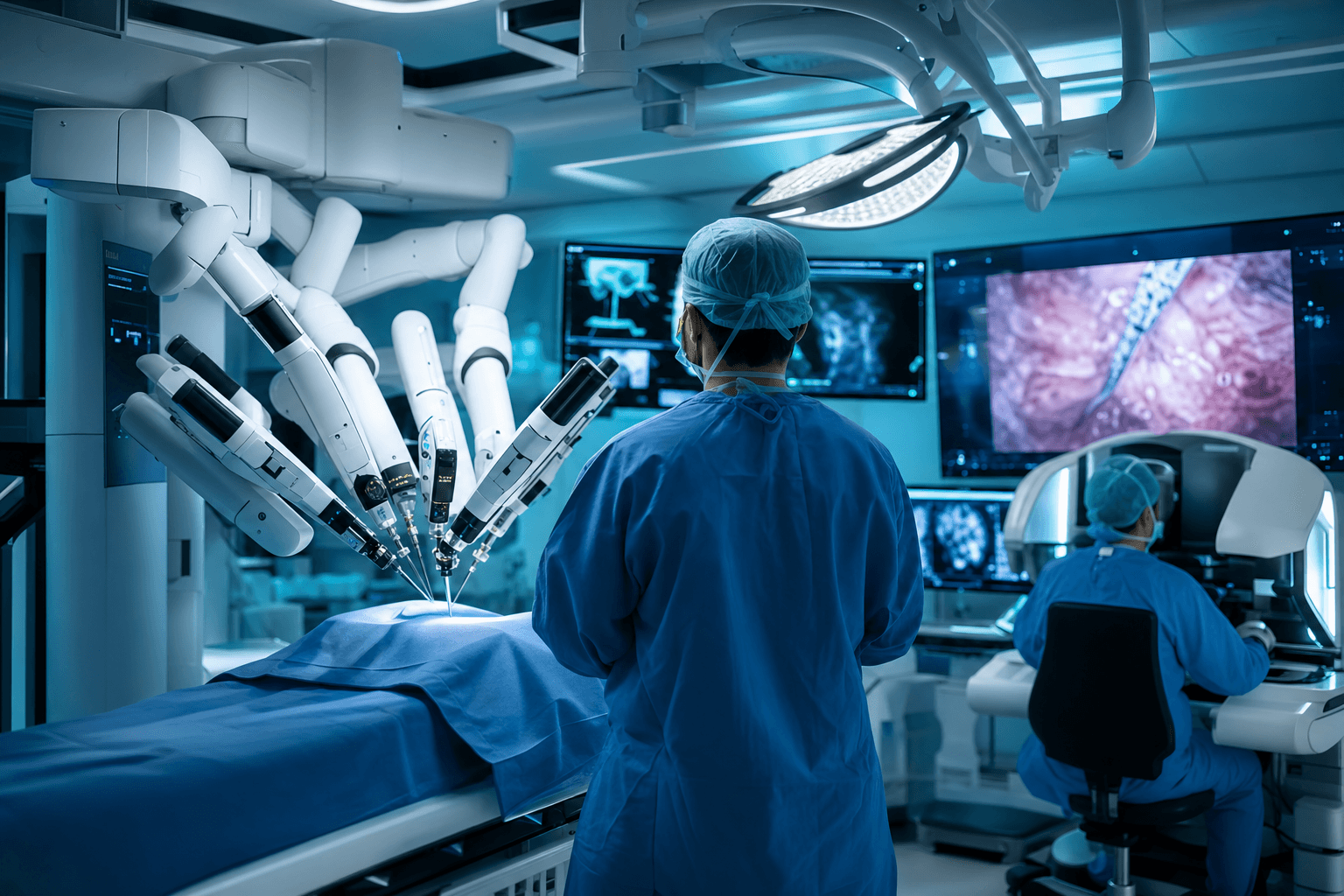
Robotic surgery is more accurately called robot assisted surgery. The surgeon sits at a console a few metres from the operating table, viewing a magnified, high definition 3D image of the surgical field. Their hand movements on the console controls are translated in real time into precise movements of miniaturised instruments mounted on robotic arms.
Nothing happens unless the surgeon moves. There is no autonomy, no pre-programmed cutting, and no artificial intelligence making clinical decisions in current mainstream systems. If the surgeon takes their hands off the controls, the instruments freeze in place. Think of the robot as an extremely sophisticated extension of the surgeon's hands, not a replacement for them.
What the machine actually adds
If the surgeon is still doing the operating, why bother with the robot at all? The system contributes several things human hands and standard laparoscopic tools cannot:
- Tremor filtration: natural hand tremor is electronically removed, so instrument tips move with steadiness no human can match.
- Motion scaling: a 3 centimetre hand movement can be scaled down to a 1 centimetre instrument movement, allowing very fine work.
- Wristed instruments: the instrument tips bend and rotate with more freedom than a human wrist, useful when suturing deep inside the pelvis or chest.
- Stable 3D vision: the camera is held perfectly still and shows depth, unlike the flat 2D image of conventional keyhole surgery.
These advantages matter most in confined spaces such as the prostate, the rectum, the uterus, and parts of the chest, which is why urology, gynaecology, and colorectal surgery adopted the technology first.
How a typical procedure unfolds
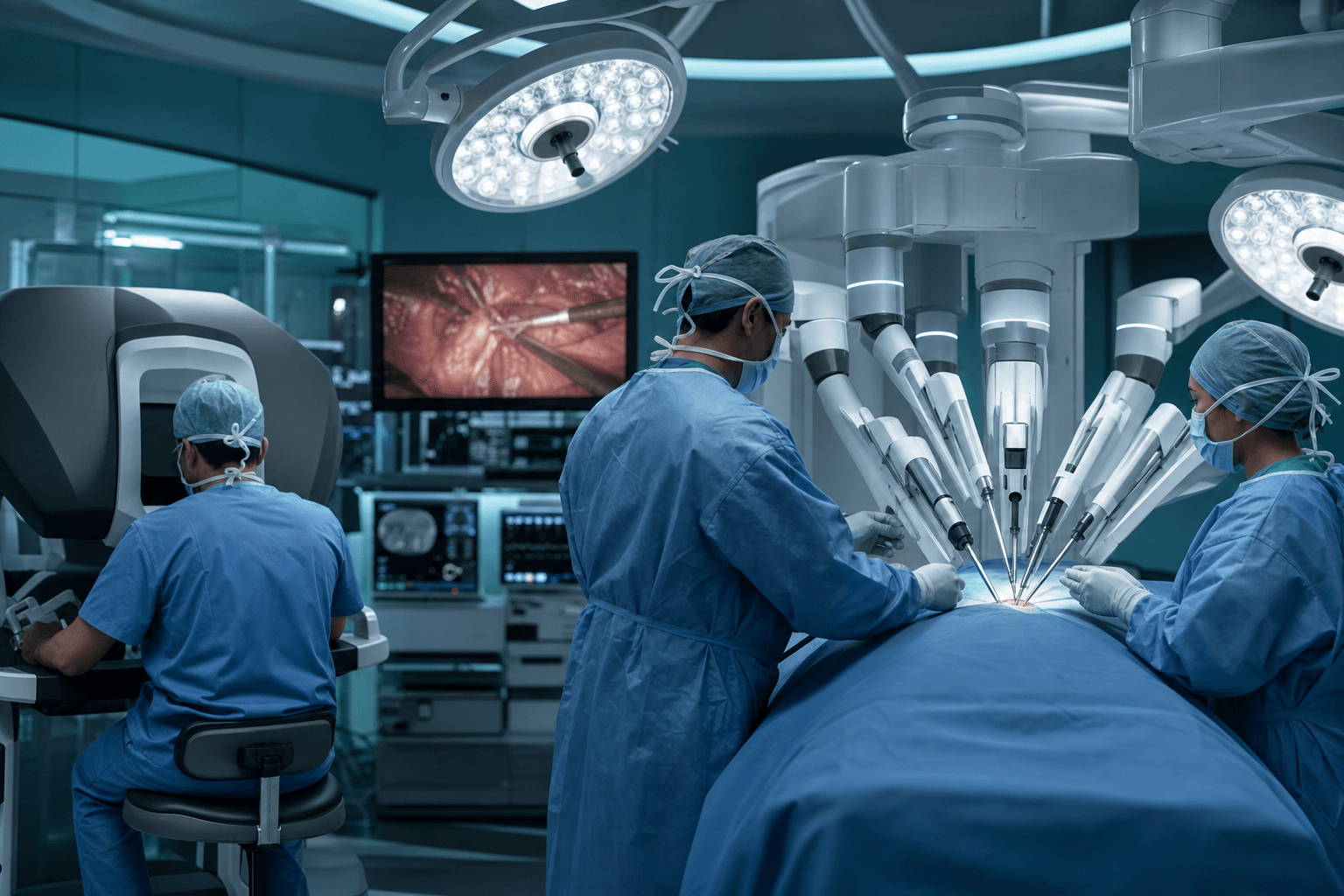
From the patient's perspective, a robot assisted operation looks much like standard keyhole surgery. You receive a general anaesthetic. The team makes a small number of incisions, usually between 8 and 12 millimetres each, and inserts ports through which the camera and instruments pass. The robotic arms are then docked to those ports.
The surgeon performs the operation from the console while a bedside assistant, a scrub nurse, and the anaesthetic team remain at the table throughout. If anything requires it, the team can undock the robot within moments and continue laparoscopically or convert to open surgery. That fallback plan is discussed and rehearsed, not improvised.
Common myths, quickly addressed
A few misconceptions come up repeatedly in clinic conversations:
- "The robot can malfunction and injure me." Systems have multiple redundant safety checks, and the instruments stop rather than move unpredictably when a fault is detected. Adverse events attributable to device failure are rare and closely monitored by regulators.
- "A junior person might be operating." Console surgeons complete structured training, simulation hours, and proctored cases before operating independently. Credentialing is specific to robotic surgery, not assumed from general surgical experience.
- "Robotic always means better." Not necessarily. For some procedures the evidence shows clear benefit; for others, outcomes are similar to well performed laparoscopy. A good surgeon will tell you honestly which category your operation falls into.
What this means for patients in Mauritius
Robotic platforms have historically been concentrated in large hospitals in Europe, the United States, and Asia, and many Mauritian patients first encounter the technology when researching treatment abroad, particularly in India or South Africa. The regional picture is changing as systems become smaller and less expensive, and private healthcare groups across the Indian Ocean region are watching the market closely. Independent coverage of medical technology in the region, including platforms like medtech.mu, can help patients follow which capabilities are actually available locally rather than relying on marketing claims.
What should you do with this knowledge? If you are offered a robot assisted procedure, ask three questions: how many of these operations has the surgeon personally performed, what is the plan if the team needs to convert to another approach, and what does the evidence say for your specific condition. Then discuss the answers with a qualified doctor who knows your full medical history. This article is education, not medical advice, and no technology choice should ever be made without that personal consultation.
Robot assisted surgery is precision medicine you can understand. Explore the wider Medtech health ecosystem.